Contrast Reactions and Pre-Medication

Prophylaxis Guidelines for Contrast Allergies
What type of adverse contrast reaction did the patient experience?
| Type of Adverse Contrast Reaction | Recommended Response |
|---|---|
| Non-allergic Reaction | No prophylaxis required. |
| Immediate Hypersensitivity Reaction | Prophylaxis contingent upon severity of reaction. (See Algorithm for next steps) |
| Unknown Reaction | Prophylaxis contingent upon date of reaction and type of contrast used. (See Algorithm for next steps) |
| Delayed Hypersensitivity Reaction | Reactions that occur 1 hour or later post injection. Prophylaxis and performance of CT contingent on reaction details. (See Algorithm for next steps) |
Non-Allergic Reaction Severity Definitions
Mild
- Isolated self-resolving nausea/vomiting
- Transient flushing, warmth, chills
- Headache, dizziness, anxiety, altered taste
- Mild hypertension
- Vasovagal reaction that resolves spontaneously
Moderate
- Protracted but isolated nausea or vomiting
- Hypertensive urgency
- Isolated chest pain
- Vasovagal reactions that require and are responsive to treatment
Severe
- Arrhythmias
- Convulsions or seizures
- Hypertensive emergencies
- Vasovagal reaction resistant to treatment
No prophylaxis required for any severity level.
Hypersensitivity Reaction Severity Definitions
Mild
- Localized itching or hives (less than 50% body surface area)
- Itchy or scratchy throat
- Nasal congestion, sneezing, redness around eyes, runny nose
Moderate
- Diffuse hives (rapidly spreading/greater than 50% body surface area)
- Facial angioedema, throat tightness/hoarseness without stridor
- Wheezing, bronchospasm without hypoxia
Severe
- Reaction involving 2 or more moderate symptoms
- Anaphylaxis
- Facial angioedema with shortness of breath
- Throat tightness/hoarseness with stridor, (laryngeal edema)
- Wheezing, bronchospasm with hypoxia
- Low blood pressure
CT Iodinated Contrast Media (ICM) Prophylaxis Algorithm
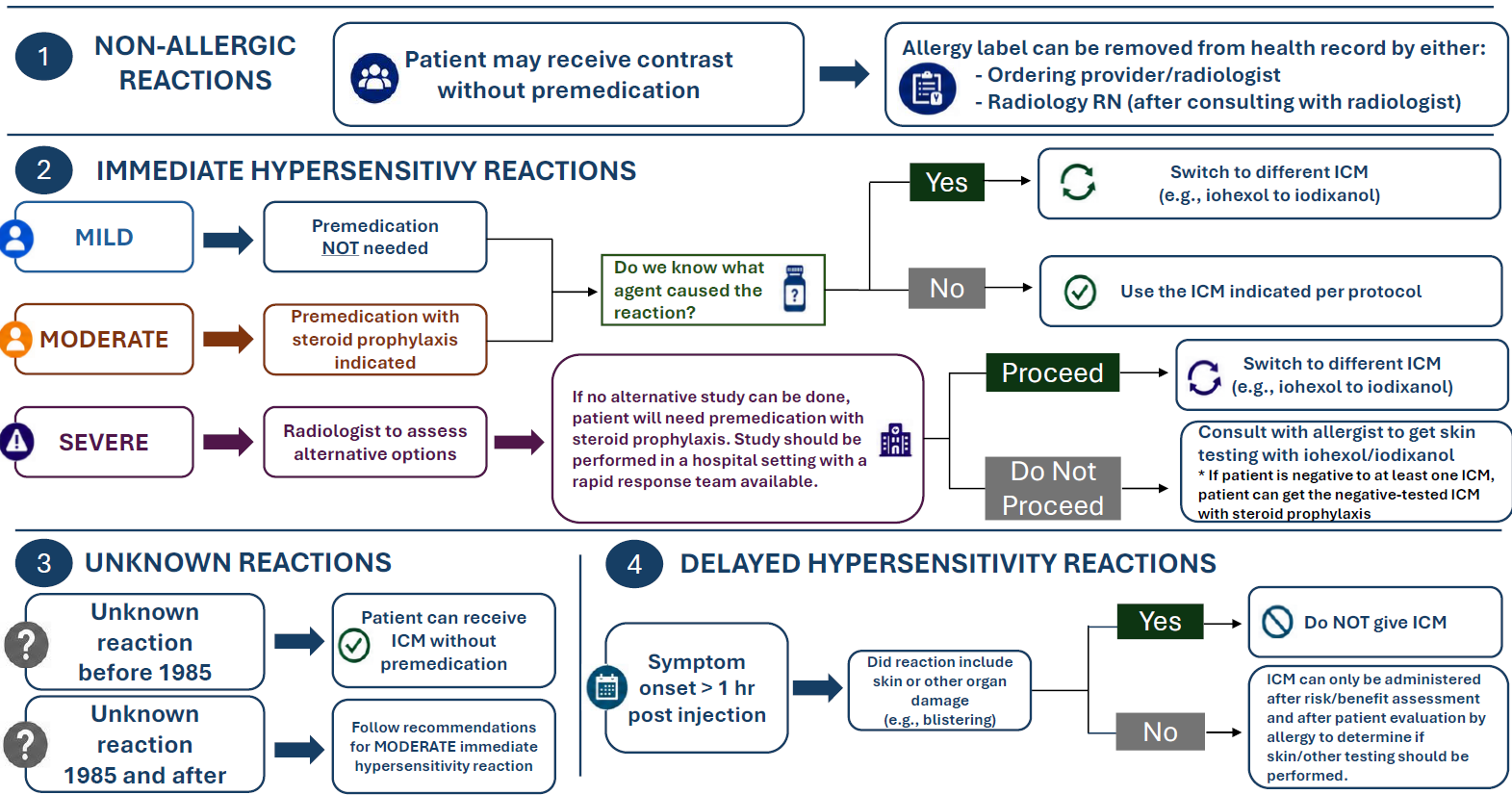
- Patient may receive contrast without medication.
- Allergy label can be removed from health record by either:
- Ordering provider/radiologist
- Radiology RN (after consulting with radiologist)
Mild
- Premedication not needed
- Do we know what agent caused the reaction?
- Yes – Switch to different ICM (e.g., iohexol to iodixanol).
- No – Use the ICM indicated per protocol.
Moderate
- Premedication with steroid prophylaxis indicated
- Do we know what agent caused the reaction?
- Yes – Switch to different ICM (e.g., iohexol to iodixanol).
No – Use the ICM indicated per protocol.
- Yes – Switch to different ICM (e.g., iohexol to iodixanol).
Severe
- Radiologist to assess alternative options
- If no alternative study can be done, patient will need premedication with steroid prophylaxis. Study should be performed in a hospital setting with a rapid response team available.
- Proceed – Switch to different ICM (e.g., iohexol to iodixanol).
- Do not proceed – Consult with allergists to get skin testing with iohexol/iodixanol. If patient is negative to at least one ICM, patient can get the negative-tested ICM with steroid prophylaxis.
- Unknown reaction before 1985, then patient can receive ICM without premedication
- Unknown reaction 1985 and after, then follow recommendations for moderate immediate hypersensitivity reaction
- Symptom onset is greater than one hour post injections.
- Did reaction include skin or other organ damage (e.g., blistering)?
- Yes – Do not give ICM.
- No – ICM can only be administered after risk/benefit assessment and after patient evaluation by allergy to determine if skin/other testing should be performed.
MR Gadolinium-Based Contrast Agent (GBCA) Prophylaxis Algorithm
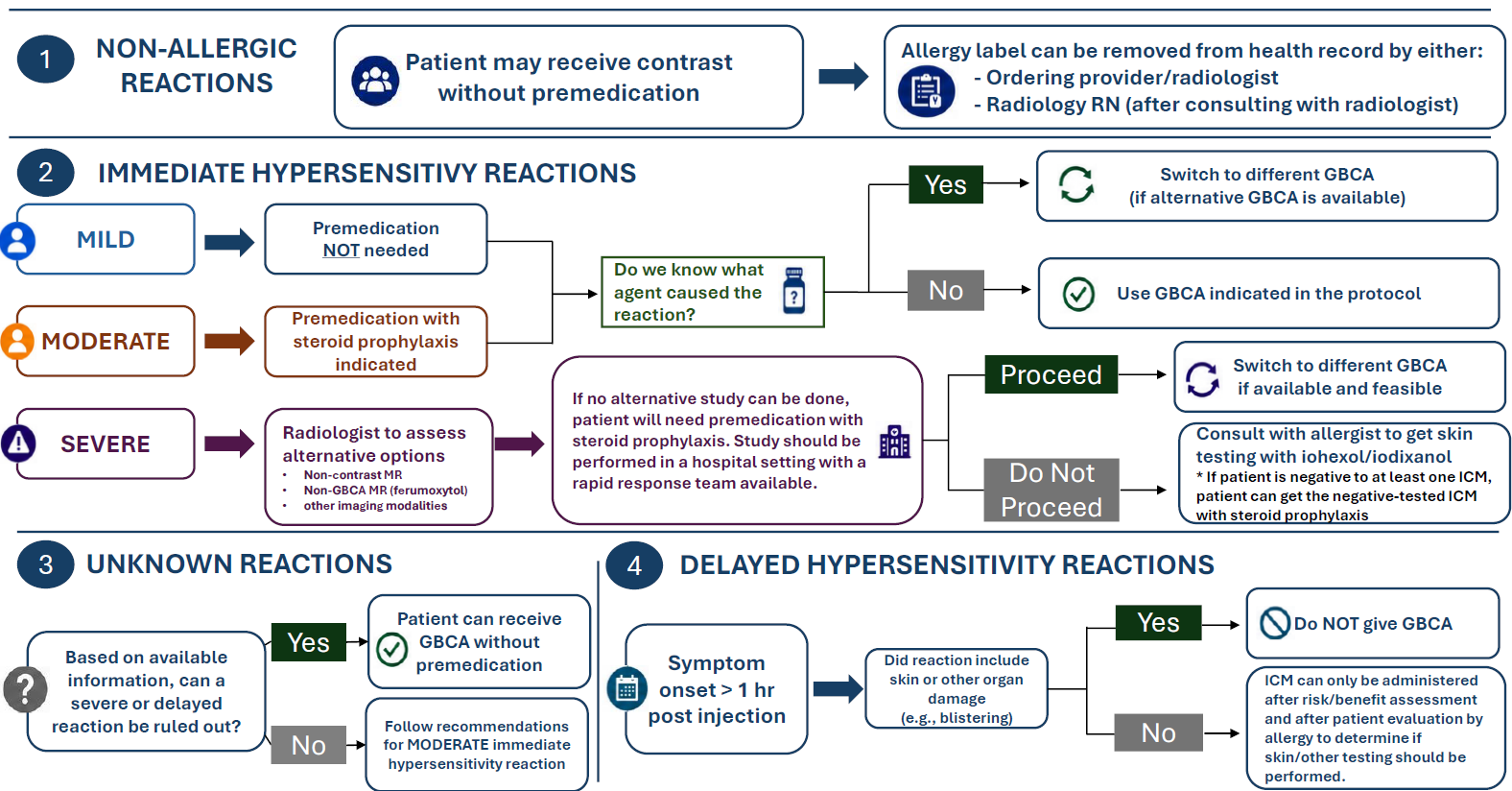
- Patient may receive contrast without medication.
- Allergy label can be removed from health record by either:
- Ordering provider/radiologist
- Radiology RN (after consulting with radiologist)
Mild
- Premedication not needed
- Do we know what agent caused the reaction?
- Yes – Switch to different GBCA (if alternative GBCA is available).
- No – Use GBCA indicated in the protocol.
Moderate
- Premedication with steroid prophylaxis indicated
- Do we know what agent caused the reaction?
- Yes – Switch to different GBCA (if alternative GBCA is available).
- No – Use GBCA indicated in the protocol.
Severe
- Radiologist to assess alternative options:
- Non-contrast MR
- Non-GBCA MR (ferumoxytol)
- Other imaging modalities
- If no alternative study can be done, patient will need premedication with steroid prophylaxis. Study should be performed in a hospital setting with a rapid response team available.
- Proceed – Switch to different GBCA (if alternative GBCA is available).
- Do no proceed – Consult with allergist to get skin testing with alternative GBCA. IF patient is negative to at least one GBCA, patient can get the negative-tested GBCA with steroid prophylaxis.
- Based on available information, can a severe or delayed reaction be ruled out?
- Yes – Patient can receive GBCA without premedication.
- No – Follow recommendations for moderate immediate hypersensitivity reaction.
- Symptom onset is greater than one hour post injection.
- Did reaction include skin or other organ damage (e.g., blistering)?
- Yes – Do not give GBCA.
- No – ICM can only be administered after risk/benefit assessment and after patient evaluation by allergy to determine if skin/other testing should be performed.
Resources
Updated June 2026
Pre-medication Policy for Patients Receiving Chronic Corticosteroid Therapy
Purpose
This document provides guidance for technologists and physicians managing patients who require corticosteroid premedication for a prior contrast allergy and who are already receiving corticosteroid therapy for another clinical indication.
This guidance is based on recommendations from the American College of Radiology (ACR) Manual on Contrast Media and supporting endocrine literature. Clinical management should be individualized based on patient-specific factors.
Background
The ACR Manual on Contrast Media provides general guidance for premedication in patients receiving chronic corticosteroid therapy. While the manual notes that premedication dosing “may be modified” in these patients, there is limited evidence supporting specific dosing adjustments.
General Principles:
- Patients receiving only Physiologic (Replacement) corticosteroid dosing generally do not require adjustment to standard premedication dosing.
- Patients already receiving Supraphysiologic (Therapeutic) corticosteroid dosing may require adjustment of the standard premedication regimen.
Corticosteroid Dose Categories
- Physiologic (Replacement) Corticosteroid Dosing
- Replacement dosing refers to glucocorticoid doses equivalent to normal daily cortisol production.
- See UpToDate Comparison of Systemic Glucocorticoid Preparations for dose equivalency
| Approximate Physiologic Daily Dose Corticosteroid | Approximate Physiologic Daily Dose |
|---|---|
| Hydrocortisone | 15–25 mg/day |
| Prednisone / Prednisolone | 4–6 mg/day |
| Methylprednisolone | 3–5 mg/day |
| Dexamethasone | 0.25–0.5 mg/day |
- Supraphysiologic (Therapeutic) Corticosteroid Dosing
- Any corticosteroid dose above physiologic replacement levels is considered therapeutic or supraphysiologic dosing.
Guidance for Premedication Adjustment
Patients on Physiologic (Replacement) Dose Steroids
(Doses equal to or below hydrocortisone 15-25 mg per day, or equivalent)
- No dose adjustments to premedication corticosteroids are made
Patients on Supraphysiologic (Therapeutic) Dose Steroids
(Doses equal to or below hydrocortisone 15-25 mg per day, or equivalent)
- Providers may consider reducing the total premedication corticosteroid dose by an
amount equivalent to the patient’s baseline daily corticosteroid dose. - Adjustments should be individualized based on clinical judgment, patient condition,
and risk assessment.
Delayed Imaging
If imaging is delayed after initiation of corticosteroid premedication:
- Patients should ideally receive at least 4–5 hours of corticosteroid therapy prior to contrast administration.
- Repeat corticosteroid doses may be administered every 4–8 hours until contrast exposure, when clinically appropriate.
Resources
- Abe S, Fukuda H, Tobe K, Ibukuro K. Protective effect against repeat adverse reactions to iodinated contrast medium: Premedication vs. changing the contrast medium. Eur Radiol. 2016;26(7):2148-2154. doi:10.1007/s00330-015-4028-1
- Beuschlein F, Else T, Bancos I, et al. European Society of Endocrinology and Endocrine Society Joint Clinical Guideline: Diagnosis and Therapy of Glucocorticoid-induced Adrenal Insufficiency. J Clin Endocrinol Metab. 2024;109(7):1657-1683. doi:10.1210/clinem/dgae250
- Husebye ES, Pearce SH, Krone NP, Kämpe O. Adrenal insufficiency. Lancet. 2021;397(10274):613-629. doi:10.1016/S0140-6736(21)00136-7
- Park HJ, Park JW, Yang MS, et al. Re-exposure to low osmolar iodinated contrast media in patients with prior moderate-to-severe hypersensitivity reactions: A multicentre retrospective cohort study. Eur Radiol. 2017;27(7):2886-2893. doi:10.1007/s00330-016-4682-y
- ACR Manual on Contrast Media. American College of Radiology. Updated 2025. Accessed March 31, 2026. https://www.acr.org/clinical-resources/clinical-tools-andreference/contrast-manual.
Updated April 2026